(BMJ)—A 24-yo Filipino man presented w/ a 1-mo hx of a rapidly growing tender mass on his chest. Exam: vital signs WNL; 7x6-cm smooth, immobile, firm mass over upper sternum, w/ mild erythema, + cervical nodes. CT confirmed the dx. What is it?

|
Lipoma
|
|
Actinomycosis
|
|
Lymphoma
|
|
Tuberculosis
|
|
Chondrosarcoma
|
(BMJ)—A 34-yo woman presented w/ a 9-day hx of progressive bilateral limb weakness and mild dysphagia w/ fluids. Exam: periorbital rash. Grade 3-4/5 bilateral proximal limb and neck flexor weakness. Deep tendon reflexes and sensation intact. Labs: creatine kinase elevated; positive antinuclear matrix protein 2 antibody; weakly positive antinuclear antibody (1:80); negative anti-dsDNA antibody. MRI: hyperintensities in thigh muscles. What is the dx?

|
Thyrotoxic periodic paralysis
|
|
Systemic lupus erythematosus
|
|
Inclusion body myositis
|
|
Myasthenia gravis
|
|
Dermatomyositis
|
(BMJ)—An 11-yo boy w/ autism who ate only potato-containing foods presented w/ bilateral blurred vision, eye pain, and nyctalopia for several weeks. Exam: visual acuity 20/60 in both eyes; superficial punctate keratopathy; severe conjunctival xerosis. What is the dx?

|
Vitamin A deficiency
|
|
Episcleritis
|
|
Hypothyroidism
|
|
Vitamin E deficiency
|
|
Sjögren syndrome
|
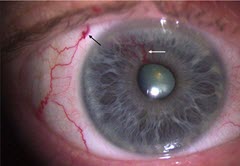
(BMJ)—A 73-yo man presented w/ a vascular lesion in his R eye. Exam: tortuous dilated vessel emerging from iris root to pupillary margin, w/ associated episcleral vessel. What is the dx?
|
Proliferative diabetic retinopathy
|
|
Arteriovenous malformation
|
|
Ocular ischemic syndrome
|
|
Uveitis
|
|
Retinal vein occlusion
|