-
Screen for anxiety/related sx in suspect pts, assess suicide risk - Suicide risk ↑1.7-2.5x in anxiety/related dz
- Consider 2-question screening (“Do you feel anxious, nervous, on edge? Do you have uncontrollable worry?”) or other tool1
- DSM-5 suggests Level 1 screening for anxiety sx, score ≥2 warrants further eval2
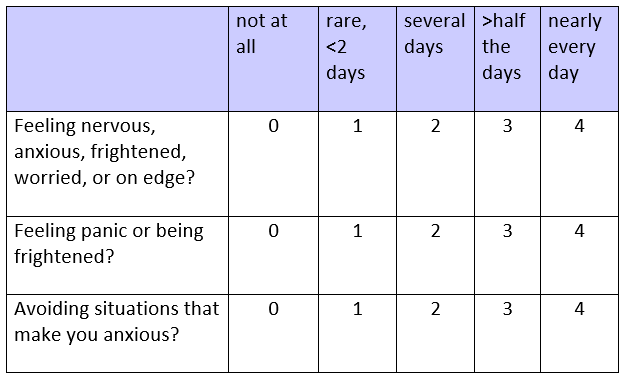
DSM-5 Level 1 Screen: During the past 2wk, how often have you been bothered by these? Conduct differential dx, assess comorbidity - R/o anxiety d/t medical or other/comorbid psych dz: panic disorder, agoraphobia, specific phobia, social anxiety disorder, PTSD, OCD, etc
- >50% of those w/ anxiety disorder have multiple anxiety disorders;1,3 20% to 60% have MDD;1,3 52%, bipolar; 47%, ADHD;1 50%, personality disorder3
- R/o substance abuse (incl caffeine), 25% have alcohol use disorder3
- R/o med effect (levothyroxine, ADHD stimulants, etc)
- Consider medical dz (hyperthyroid, cardiopulmonary dz) via H&P, labs, per ADAC, WCA;1,3 medical dz may cause anxiety sx, but anxiety pts also have ↑prevalence of medical dz
Diagnose GAD by DSM-5 criteria (all req'd)2 - Excessive anxiety/worry about multiple events/activities most days, ≥6mo
- Difficult to control worry
- Assoc w/ 3+ of these: restlessness (keyed-up, on edge), fatigue, difficulty concentrating, irritability, muscle tension, abnl sleep
- Causes significant distress/impairment in social/occupational setting
- Not secondary/attributable to other med dz, psych disorder, substance/drug
Footnotes 1 ADAC 2014. Katzman MA, et al. Canadian Clinical Practice Guidelines for the Management of Anxiety, Posttraumatic Stress and Obsessive-Compulsive Disorders. BMC Psychiatry. 2014;14(Suppl 1):S1-83. PubMed abstract | Free full-text PDF
Other anxiety screening tools include:
• GAD7 questionnaire – available in epocrates calculators
• Two-question screening: During the past 4wk, have you been bothered by feeling worried, tense, or anxious most of the time? Are you frequently tense, irritable, and having trouble sleeping?
Hx to include review of systems, prescribed meds, OTC agents, EtOH use, caffeine intake, illicit drug use, and degree of functional impairment.
Lab eval to consider: CBC, lytes, FBG, TSH, lipids, LFTs, and urine drug screen (if suspected).
2 APA 2013. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Association, 2013.
Follow-up eval w/ positive Level 1 screening is Level 2 screening w/ PROMIS Emotional Distress—Anxiety—Short Form.
3 WCA 2003. Allgulander C, et al. Recommendations for the Long-Term Treatment of Generalized Anxiety Disorder. CNS Spectr. 2003. Aug;8(8 Suppl1):53-61. PubMed abstract -
GAD dx, awaiting initial tx
Consider treating substance abuse first, if present - Treat harmful/dependent substance use before GAD1
- Nonharmful substance use not a contraindication to GAD tx, may be complication of GAD, per NICE1
Educate about disorder, discuss tx options - Tx indicated for most who meet DSM criteria, per WFSBP2
- Educate about dz course, tx options/efficacy/side effects/latency/tolerability1-3
- Consider offering individual self-help, per ADAC;3 use self-help in pts not responsive to education alone, per NICE1
- Little evidence for additive effect of CBT + meds, but pharmacologic tx and psychologic tx “partners, not alternatives,” per WFSBP2
- Factor into tx decision: pt pref, drug side effects/latency, pt convenience,2 motivation, engagement; severity of dz; clinician skills/experience; availability of psychological treatments; prior tx response; comorbid med/psych dz;3 cost2
Footnotes 1 NICE 2011. Generalised Anxiety Disorder and Panic Disorder in Adults: Management. NICE Guideline (CG113). London: National Institute for Health and Clinical Excellence (UK). Published Jan 26, 2011. Last updated: 15 June 2020. Free full-text PDF
2 WFSBP 2009. Bandelow B, et al. World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for the Pharmacological Treatment of Anxiety, Obsessive-Compulsive and Posttraumatic Stress Disorders. World J Biol Psychiatry. 2009. Jul 12;3(4):171-199. Free full-text PDF
3 ADAC 2014. Katzman MA, et al. Canadian Clinical Practice Guidelines for the Management of Anxiety, Posttraumatic Stress and Obsessive-Compulsive Disorders. BMC Psychiatry. 2014;14(Suppl 1):S1-83. PubMed abstract | Free full-text PDF
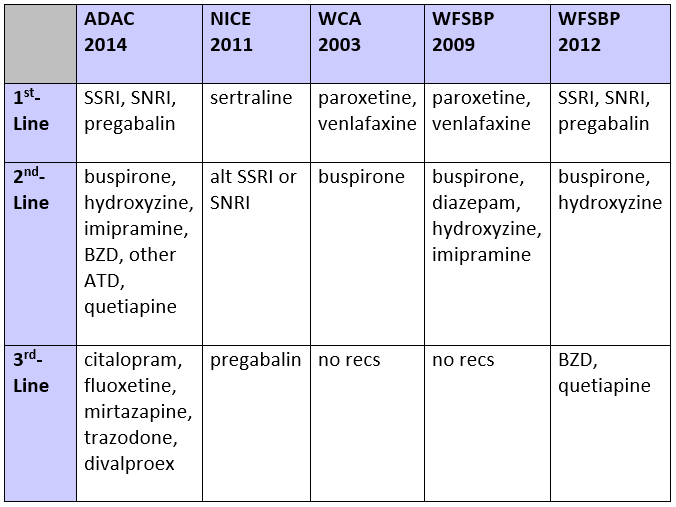
Use SSRI or SNRI as 1st-line agent of choice - Paroxetine and escitalopram (SSRI), venlafaxine and duloxetine (SNRI) approved for GAD; off-label sertraline use common, encouraged by ADAC,1 NICE,2 and WFSBP3
- Efficacy: SSRI=SNRI (though escitalopram < venlafaxine in 1 study)1
- Discuss prior to drug start: side effects, drug interactions, latency (2-8wk), tx duration, w/d after cessation, etc2
- If pt <30 yo, warn of ↑suicide risk and monitor closely, per NICE;2 use caution if comorbid bipolar I disorder1
- Dose-response curve is flat; 75% respond to initial low dose3,4
- Use lower doses in elderly pts; latency may be longer3
- If intolerant to initial drug, consider alternative 1st-line SSRI or SNRI
- Follow-up: q2wk first 6wk, then q1mo, per ADAC;1 q2-4wk first 3mo, then q3mo, per NICE2
- HAM-A scale may be used to monitor response3,5
- Tx ≥6-24mo after remission, per WFSBP;4 ≥12mo, per NICE2
If intolerant to 1st-line SSRI/SNRI, use 2nd- & 3rd-line agents - 2nd-line options: pregabalin, per ADAC,1 NICE,2 and WFSBP;4 buspirone, per ADAC,1 WCA,5 WFSBP3,4
- TCAs, hydroxyzine also options, per ADAC,1 WFSBP,3,4 but side effects may be limiting; avoid TCA if pt suicidal;4 limit hydroxyzine to 5-wk course
- BZD can be useful for crisis tx, or in combo w/ antidepressant in short term;1,2 avoid chronic use, per NICE,2 WCA,5 WFSBP4
- Antipsychotic (eg, quetiapine) use controversial & off-label; not recommended in primary care, per NICE,2 WFSBP;4 OK for 2nd-line use, per ADAC1
Footnotes 1 ADAC 2014. Katzman MA, et al. Canadian Clinical Practice Guidelines for the Management of Anxiety, Posttraumatic Stress and Obsessive-Compulsive Disorders. BMC Psychiatry. 2014;14(Suppl 1):S1-83. PubMed abstract | Free full-text PDF
1st-line classes:
• SSRI: paroxetine, escitalopram, sertraline
• SNRI: venlafaxine, duloxetine
2nd-line classes:
• BZD: alprazolam, diazepam, lorazepam
• Other antidepressant: bupropion, vortioxetine
3rd-line:
• fluoxetine, citalopram
Alternative meds shown to be >placebo or =BZD:
• silexan (lavender oil)
• galphimia glauca extract
• passiflora
• valerian
2 NICE 2011. Generalised Anxiety Disorder and Panic Disorder in Adults: Management. NICE Guideline (CG113). London: National Institute for Health and Clinical Excellence (UK). Published Jan 26, 2011. Last updated: 15 June 2020. Free full-text PDF
3 WFSBP 2009. Bandelow B, et al. World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for the Pharmacological Treatment of Anxiety, Obsessive-Compulsive and Posttraumatic Stress Disorders. World J Biol Psychiatry. 2009. Jul 12;3(4):171-199. Free full-text PDF
4 WFSBP 2012. Bandelow B, et al. Review Article. Guidelines for the Pharmacological Treatment of Anxiety Disorders, Obsessive-Compulsive Disorder and Posttraumatic Stress Disorder in Primary Care. Int J Psychiatry Clin Pract. 2012. Jun;16(2):77-84. Free full-text PDF
Pregabalin onset occurs in the 1st few days, which is an advantage over SSRI/SNRI.
1st-line classes:
• SSRI: paroxetine, escitalopram, sertraline
• SNRI: venlafaxine (extended release preferred), duloxetine
3rd-line:
• BZD: diazepam, lorazepam
5 WCA 2003. Allgulander C, et al. Recommendations for the Long-Term Treatment of Generalized Anxiety Disorder. CNS Spectr. 2003. Aug;8(8 Suppl1):53-61. PubMed abstract
Prefers nonpharmacologic tx CBT by trained clinician is preferred psychological tx - Effectiveness of CBT=medication;1,2 50% to 60% clinically improve
- Applied relaxation also an option, per NICE, WCA;2,3 efficacy limited, per ADAC1
- HAM-A scale is available to monitor response2,4
- Tx duration: 8-12wk, per ADAC;1 6wk, per NICE;3 12wk, per WCA2
- Can be administered in individual and group settings; self-directed tools also effective1,3
Footnotes 1 ADAC 2014. Katzman MA, et al. Canadian Clinical Practice Guidelines for the Management of Anxiety, Posttraumatic Stress and Obsessive-Compulsive Disorders. BMC Psychiatry. 2014;14(Suppl 1):S1-83. PubMed abstract | Free full-text PDF
2 WCA 2003. Allgulander C, et al. Recommendations for the Long-Term Treatment of Generalized Anxiety Disorder. CNS Spectr. 2003. Aug;8(8 Suppl1):53-61. PubMed abstract
3 NICE 2011. Generalised Anxiety Disorder and Panic Disorder in Adults: Management. NICE Guideline (CG113). London: National Institute for Health and Clinical Excellence (UK). Published Jan 26, 2011. Last updated: 15 June 2020. Free full-text PDF
4 WFSBP 2009. Bandelow B, et al. World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for the Pharmacological Treatment of Anxiety, Obsessive-Compulsive and Posttraumatic Stress Disorders. World J Biol Psychiatry. 2009. Jul 12;3(4):171-199. Free full-text PDF
Combo pharmacologic tx + CBT not well supported by evidence - Trials of combined tx in adults are limited, conflicting;1 RCT showed diazepam + CBT > other options early, but not at 6mo.2 Another study showed no diff btwn buspirone combo tx and mono-tx3
- Large RCT in peds shows sertraline + CBT > either mono-tx, per ADAC1
- However, WFSBP considers CBT & pharmacologic tx as “partners, not alternatives”3
Footnotes 1 ADAC 2014. Katzman MA, et al. Canadian Clinical Practice Guidelines for the Management of Anxiety, Posttraumatic Stress and Obsessive-Compulsive Disorders. BMC Psychiatry. 2014;14(Suppl 1):S1-83. PubMed abstract | Free full-text PDF
2 WCA 2003. Allgulander C, et al. Recommendations for the Long-Term Treatment of Generalized Anxiety Disorder. CNS Spectr. 2003. Aug;8(8 Suppl1):53-61. PubMed abstract
3 WFSBP 2009. Bandelow B, et al. World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for the Pharmacological Treatment of Anxiety, Obsessive-Compulsive and Posttraumatic Stress Disorders. World J Biol Psychiatry. 2009. Jul 12;3(4):171-199. Free full-text PDF
-
Confirm dx, use alternate 1st-line agent; other tx only when all 1st-line tx fails - Reassess dx, r/o med/psych comorbidities if tx resistant;1 personality disorder seen in 80% of resistant GAD, per WCA2
- Ensure tx compliance1
- Start pharmaco-tx trial in pts resistant to CBT, per ADAC, NICE1,3
- Consider adding CBT in pts w/ partial response to pharmaco-tx1,3
- Exhaust all 1st-line pharmaco-tx before considering 2nd-/3rd-line agents1,3-5
- Consider adding buspirone (2nd-line) or antipsychotics (3rd-line) to 1st-line agents, per ADAC1
- Can consider alternative med, biologic tx (rTMS), or yoga/exercise/meditation in lieu of 3rd-line med, per ADAC1
- Refer complex tx-refractory GAD to specialty care, per NICE;3 refer if antipsychotics used, per NICE, WFSBP3,5
Footnotes 1 ADAC 2014. Katzman MA, et al. Canadian Clinical Practice Guidelines for the Management of Anxiety, Posttraumatic Stress and Obsessive-Compulsive Disorders. BMC Psychiatry. 2014;14(Suppl 1):S1-83. PubMed abstract | Free full-text PDF
1st-line classes:
• SSRI: paroxetine, escitalopram, sertraline
• SNRI: venlafaxine, duloxetine
2nd-line classes:
• BZD: alprazolam, diazepam, lorazepam
• Other antidepressant: bupropion, vortioxetine, trazodone
3rd-line:
• fluoxetine, citalopram
Alternative meds shown to be >placebo or =BZD:
• silexan (lavender oil)
• galphimia glauca extract
• passiflora
• valerian
2 WCA 2003. Allgulander C, et al. Recommendations for the Long-Term Treatment of Generalized Anxiety Disorder. CNS Spectr. 2003. Aug;8(8 Suppl1):53-61. PubMed abstract
3 NICE 2011. Generalised Anxiety Disorder and Panic Disorder in Adults: Management. NICE Guideline (CG113). London: National Institute for Health and Clinical Excellence (UK). Published Jan 26, 2011. Last updated: 15 June 2020. Free full-text PDF
4 WFSBP 2009. Bandelow B, et al. World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for the Pharmacological Treatment of Anxiety, Obsessive-Compulsive and Posttraumatic Stress Disorders. World J Biol Psychiatry. 2009. Jul 12;3(4):171-199. Free full-text PDF
5 WFSBP 2012. Bandelow B, et al. Review Article. Guidelines for the Pharmacological Treatment of Anxiety Disorders, Obsessive-Compulsive Disorder and Posttraumatic Stress Disorder in Primary Care. Int J Psychiatry Clin Pract. 2012. Jun;16(2):77-84. Free full-text PDF
1st-line classes:
• SSRI: paroxetine, escitalopram, sertraline
• SNRI: venlafaxine, duloxetine
3rd-line:
• BZD: diazepam, lorazepam
|