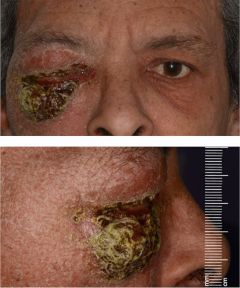
(BMJ)—A 70-yo man w/ no PMHx presented w/ sudden-onset R periorbital swelling w/o hx of trauma. Exam: mild tachycardia, afebrile; periorbital area red, swollen, indurated w/ desquamation of lower lid. His s/sx worsened over 48h despite IV abx. What is the dx?
|
Squamous cell carcinoma
|
|
Periorbital necrotizing fasciitis
|
|
Carotid cavernous fistula
|
|
Dacryoadenitis
|
|
Orbital dermoid
|
(BMJ)—A 26-yo pregnant woman at 25wk gestation who had chronic abdominal pain treated w/ hot water bottles presented w/ longstanding skin discoloration and fragility over her abdomen and thighs. Exam: reticulated red rash w/ areas of hypopigmentation. What is the dx?

|
Degos disease
|
|
Nevus anemicus
|
|
Cutis marmorata
|
|
Erythema ab igne
|
|
Livedo racemosa
|
(BMJ)—An otherwise healthy 3-mo boy had intertriginous eruption x3 days but no other sx. Other family members were not affected. Exam: well-defined red area of erythema and maceration of inguinal folds and genitals; no satellite lesions. What is the dx?

|
Granuloma gluteal infantum
|
|
Congenital syphilis
|
|
Familial benign pemphigus
|
|
Herpes simplex
|
|
Intertrigo complicated by group A strep
|